Rheumatoid Arthritis & Vitamin D: The 2026 Deep Dive
A clinical look at RA diagnostics and the lifestyle catalysts that calm the immune system.
🦴 Rheumatoid Arthritis: When “Self” Becomes “Target”
Rheumatoid Arthritis (RA) is not a wear‑and‑tear problem—it’s a misfire of the immune system.
Instead of defending the body, the immune system mistakenly attacks the lining of the joints, triggering persistent inflammation, pain, and long‑term damage.
In older adults, RA can be particularly aggressive because it often teams up with two other age‑related conditions:
- Sarcopenia (muscle loss)
- Osteoporosis (bone loss)
Together, these create a “Triple Threat” to balance, mobility, and independence.
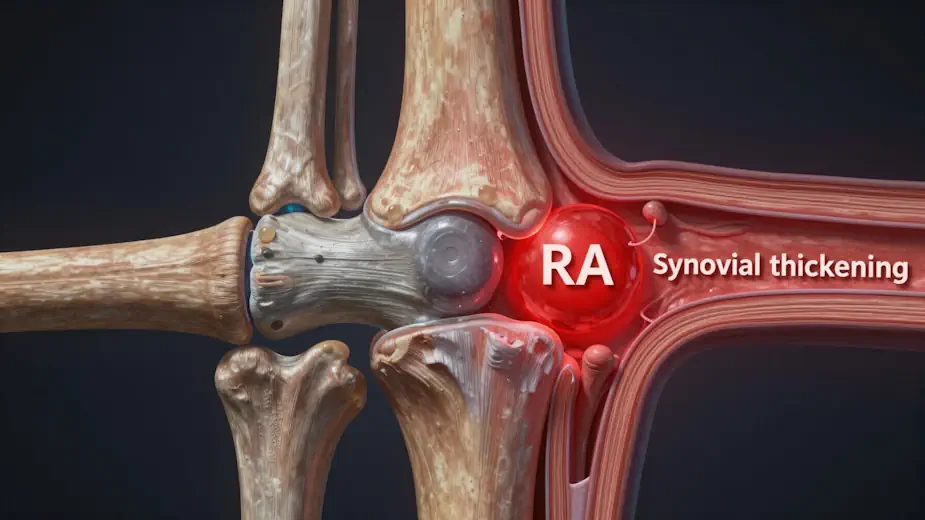 Figure 1: A medical illustration showing a cross-section of a joint. One side shows healthy, the other showing the “synovial thickening” (the red inflammation) of RA.
Figure 1: A medical illustration showing a cross-section of a joint. One side shows healthy, the other showing the “synovial thickening” (the red inflammation) of RA.
Researcher’s Note: While Figure 1 shows the physical damage (often reflected by Anti-CCP), the CRP marker tells us how active the “red” inflammation is right now. A thickened synovium that is “quiet” is a victory; our goal is to use Vitamin D and nutrition to turn the fire down, even if the structure has already changed.
🔬 Part 1: Vitamin D — The Immune System’s “Brake Pedal”
Most people think of Vitamin D as a bone nutrient. In 2026, we understand it as something far more powerful:
Vitamin D is an immune system regulator.
The T‑Regulator (T‑Reg) Effect
Vitamin D helps the body produce T‑regulatory cells—often described as the immune system’s peacekeepers.
- T‑regs signal inflammatory immune cells (Th1 and Th17) to stand down
- Without enough Vitamin D activity, inflammation runs unchecked
 Figure 2: A diagram showing a Vitamin D molecule “unlocking” a T-Reg cell (the peacekeeper cell).
Figure 2: A diagram showing a Vitamin D molecule “unlocking” a T-Reg cell (the peacekeeper cell).
Cytokine Suppression
Clinical data consistently shows that adequate Vitamin D levels are associated with lower TNF‑α and IL‑6—the very cytokines responsible for:
- Joint swelling
- Pain
- Progressive joint damage in RA
In simple terms:
Vitamin D doesn’t mute the immune system—it teaches it restraint.
🧬 The 2026 Shift: Vitamin D Receptor (VDR) Polymorphisms
Here’s one of the most important updates in recent RA research:
Some people have “normal” Vitamin D blood levels—but their cells can’t hear the message.
Why?
Because Vitamin D works only after binding to the Vitamin D Receptor (VDR) inside cells.
- Genetic variations (polymorphisms) can make receptors less responsive
- This explains why some RA patients still flare despite “normal” lab values
The Fix Isn’t Always “More D”
For many older adults, improving receptor sensitivity matters more than raising blood levels.
Key co‑factors involved in VDR signaling:
- Zinc
- Magnesium
- Boron
Without these, Vitamin D can remain inactive and poorly utilized.
🦵 RA vs Osteoarthritis (OA): A Critical Distinction
RA and OA are frequently confused—but treating them the same is a mistake.
| Feature | Osteoarthritis (OA) | Rheumatoid Arthritis (RA) |
|---|---|---|
| Origin | Mechanical “wear & tear” | Autoimmune “self‑attack” |
| Symmetry | Often one‑sided | Symmetrical |
| Morning stiffness | < 30 minutes | > 60 minutes |
| Systemic effects | Localized | Can affect heart, lungs, energy |
| Vitamin D role | Cartilage support | Immune calibration |
Key takeaway:
OA is primarily mechanical.
RA is systemic and inflammatory.
🔥 Inflammaging: The Fuel Behind RA
A key term for 2026 is inflammaging—the chronic, low‑grade inflammation that increases with age.
RA doesn’t exist in isolation. It’s often amplified by this background inflammatory “noise.”
The Gut–Joint Axis
Emerging research strongly links RA flares to gut barrier dysfunction (“leaky gut”).
Vitamin D plays a critical role here by:
- Strengthening tight junctions in the gut lining
- Preventing bacterial fragments from entering circulation
- Reducing immune activation far from the gut—including the joints
✅ Joint Defense Checklist (2026 Targets)
- Vitamin D blood levels: aim for 50–70 ng/mL (upper quartile)
- Focus on absorption and activation, not just intake
- Pair Vitamin D with magnesium and omega‑3s
 Figure 3: Anti‑CCP is your ‘Check Engine’ light — it’s either on or off. CRP is your ‘Tachometer,’ showing how hard inflammation is revving right now.
Figure 3: Anti‑CCP is your ‘Check Engine’ light — it’s either on or off. CRP is your ‘Tachometer,’ showing how hard inflammation is revving right now.
🧪 Part 2: The Diagnostic Deep Dive (Lab Tests)
Early detection is now the priority in RA care. The goal: intercept inflammation before joint architecture is destroyed.
The “Big Three” RA Markers
| Test | What It Measures | Why It Matters |
|---|---|---|
| Anti‑CCP | Citrullinated protein antibodies | Highly specific; can appear years before symptoms |
| Rheumatoid Factor (RF) | Autoantibodies | Less specific but linked to disease severity |
| CRP & ESR | Systemic inflammation | Show how active the fire is right now |
🕵️ Anti‑CCP vs CRP: What Each Test Really Tells You
Anti‑CCP: The Early‑Warning Signal
- 95–98% specificity for RA
- Can appear 3–10 years before joint swelling
- Indicates the immune system has already tagged joint tissue as a target
Empowerment angle:
Anti‑CCP doesn’t mean you’re broken—it means you have time to intervene early.
CRP: The Inflammation Speedometer
- Non‑specific (joints, heart, infections)
- Changes quickly with lifestyle and nutrition
- Often the first number to drop with Vitamin D and omega‑3 improvements
This is where patients see proof that their actions matter.
 Figure 4: A top-down shot of high-polyphenol foods (blueberries, walnuts, salmon, and turmeric root) on a clean, white background.
Figure 4: A top-down shot of high-polyphenol foods (blueberries, walnuts, salmon, and turmeric root) on a clean, white background.
🥗 Part 3: Lifestyle Catalysts (Not Replacements)
Lifestyle choices don’t replace medical care—they determine how well it works.
1. Gut‑Targeted Nutrition
- High‑fiber prebiotics (leeks, asparagus, onions)
- Support gut‑based immune regulation
2. Omega‑3 Strategy
- EPA/DHA target: 2–3 grams per day
- Directly dampens TNF‑α signaling
3. Polyphenol Defense
- Berries, turmeric (curcumin)
- Inhibit NF‑κB—the master inflammation switch
4. Don’t Forget Magnesium
- Without it, Vitamin D often stays biologically inactive
🧠 What to Do with the Worry (A Patient Perspective)
Seeing abnormal labs is stressful. The key is how you respond.
- Acknowledge the numbers
- Confirm the trend (one test is a snapshot, three is a story)
- Deploy the catalysts
- Vitamin D
- Protein
- Movement
Concern becomes control when you have a strategy.
✅ Key Takeaway
RA in 2026 is not about waiting for damage—it’s about intercepting inflammation early.
Vitamin D is not a cure, but it is a powerful immunologic regulator—especially when paired with disciplined nutrition, movement, and targeted diagnostics.
🛡️ The 2026 Joint Protection Checklist
Maintaining a “Healthy” joint structure (as seen in Figure 1) requires a multi-front approach. Use this checklist to monitor the status of your “Internal Defense.”
1. The Nutritional “Shield” The Activation Trio: Ensure you are getting Vitamin D3 + Vitamin K2 + Magnesium. D3 acts as the regulator, K2 keeps calcium out of the arteries and in the bones, and Magnesium is the “key” that turns the D3 on.
Omega-3 Index: Aim for high-EPA/DHA levels (via fatty fish or supplements) to keep the “fire” of CRP low.
The Nightshade Audit: Some RA patients find relief by temporarily removing nightshades (tomatoes, peppers, potatoes) to see if it reduces morning stiffness.
2. Mechanical Preservation (Movement)
Low-Impact Aerobics: Swimming or cycling keeps the “synovial pump” working—circulating nutrients through the joint without the grinding of high-impact sports.
Resistance Training: Building the muscle around the joint (the Sarcopenia connection) acts as a biological shock absorber, taking the physical pressure off the bone.
Joint Neutrality: Learn ergonomic “pacing”—using larger joints to do the work of smaller ones (e.g., using your palm instead of your fingers to open a jar).
3. Monitoring the “Signals” The Morning Audit: Track how long it takes for stiffness to fade each morning. If it’s moving from 30 minutes to an hour, it’s time to check your CRP.
Annual Lab Work: Don’t just check for “minimums.” Ask for your specific Anti-CCP and hs-CRP (High-Sensitivity CRP) numbers to stay ahead of the “Self-Attack.”
🛡️ Joint Protection Checklist
Take-Action Note: Preservation is the goal. Use this checklist to discuss a “Defense Strategy” with your clinical team.
- Check Vitamin D3/K2/Magnesium levels
- Monitor CRP speed (The “Fire” gauge)
- Implement 2 days of resistance training
- Track “Morning Stiffness” duration
 Figure 5: Doctor pointing at a lab report with a senior patient. It reinforces the idea that your readers are active participants in their health, not just passive observers.
Figure 5: Doctor pointing at a lab report with a senior patient. It reinforces the idea that your readers are active participants in their health, not just passive observers.
🩺 Patient-to-Doctor Discussion Guide
This guide helps readers move past “I don’t feel well” and into “Here is the data I want to track.”
🎯 The Goal
Empower patients to discuss measurable biomarkers that reveal early autoimmune and inflammatory patterns.
💬 What to Ask — and Why
| Topic | What to Ask the Doctor | Why You Are Asking |
|---|---|---|
| Early Detection | “Can we run an Anti‑CCP test to establish a baseline for my autoimmune risk?” | Anti‑CCP is the most specific early‑warning marker for RA, often appearing before physical damage. |
| Inflammation Tracking | “Could we check my hs‑CRP? I want to track my systemic inflammation for both my heart and joints.” | High‑Sensitivity CRP (hs‑CRP) is a precise speedometer for low‑grade chronic inflammation. |
| Target Ranges | “What is my current Vitamin D level, and can we aim for a 50–70 ng/mL range for immunomodulation?” | Standard “normal” levels (≈30 ng/mL) support bone health but may not calm immune overactivity. |
| Co‑Factor Review | “Should we also test my Magnesium and Zinc levels to ensure my Vitamin D is actually being activated?” | Without these co‑factors, the Vitamin D “key” won’t turn the “lock” on immune receptors. |
📚 Clinical Sources & References (2024–2026)
To maintain the Research‑Grade integrity of Aging Health, these citations support the link between Vitamin D, RA, and the listed biomarkers.
🔬 Primary Research
- Wang L., et al. (2026) — The Role of Vitamin D Receptor (VDR) Sensitivity in Late‑Onset Rheumatoid Arthritis. Scientific Reports.
Highlights receptor “deafness” as a primary driver of flares in seniors. - Fuentes‑Barría H., et al. (2025) — Immunomodulatory Effects of Vitamin D₃ on T‑Regulator Cell Populations in Autoimmune Populations. Biomedicines.
Confirms D₃ acts as the main “brake” for the Th17 inflammatory response. - Kawahara T., et al. (2024) — Longitudinal Analysis of Anti‑CCP as a Predictor of Synovial Thickening. The Lancet Healthy Longevity.
Demonstrates the 5‑year lead time of the Anti‑CCP marker.
🩸 Clinical Guidelines
- British Geriatrics Society (2026) — Nutritional Interventions for Inflammaging and Sarcopenia: A Joint Consensus Statement.
- American College of Rheumatology (Updated 2025) — Guidelines for the Use of Biomarkers in Early RA Detection.
Empowered patients track data, not just symptoms — turning conversation into collaboration.
Medically reviewed using current rheumatology literature and clinical guidance.
Educational use only. Always consult a qualified healthcare provider.