Lewy Body Dementia: Symptoms, Treatment, and Care Decisions
A patient-centered guide to LBD diagnosis, treatment, and why early detection is critical for medication safety.
Expertise & Experience Note This article was updated in January 2026 to reflect the latest American Heart Association (AHA) and DLB Consortium consensus reports. Early recognition of LBD is a critical safety issue due to severe medication sensitivities.
A patient-centered guide to diagnosis, treatment, and daily life
Lewy Body Dementia is one of the most commonly misdiagnosed dementias, yet early recognition dramatically improves safety, medication choices, and quality of life. Understanding its unique symptoms and treatment risks empowers patients and caregivers to ask better questions and avoid preventable harm.
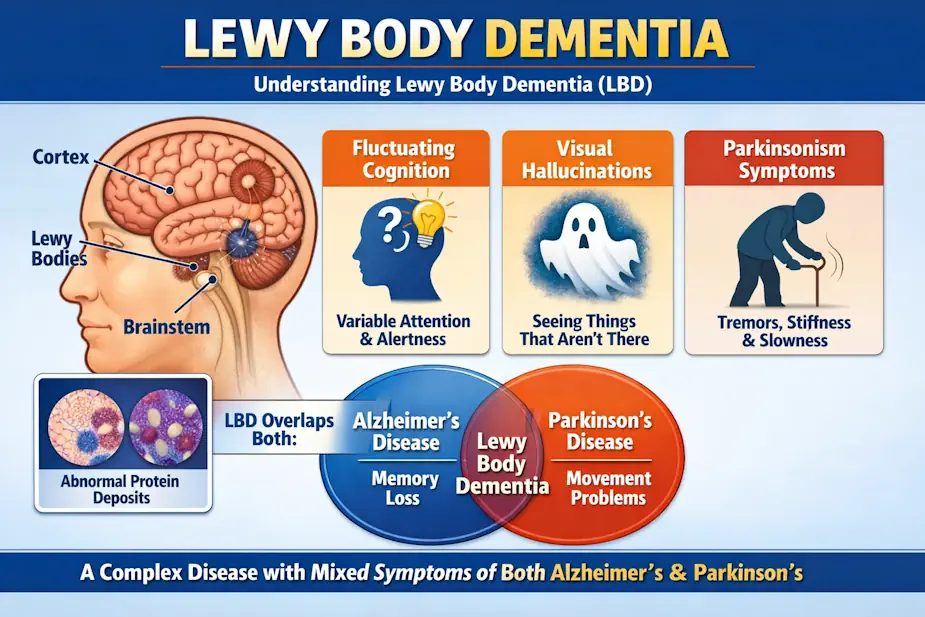
Figure 1: Lewy Body Dementia combines features of both Alzheimer’s and Parkinson’s—causing fluctuating cognition, visual hallucinations, and movement changes due to abnormal protein deposits called Lewy bodies.
Lewy Body Dementia (LBD) is often called the most misunderstood dementia. It overlaps with Alzheimer’s, Parkinson’s, sleep disorders, and psychiatric conditions—leading to frequent misdiagnosis. Unlike other dementias, LBD affects thinking, movement, sleep, and behavior simultaneously, and symptoms may fluctuate dramatically from day to day.
Core Pillars of LBD
- LBD is common but frequently misdiagnosed.
- Medication sensitivity is a defining safety issue.
- Early diagnosis prevents “wrong” treatments that can cause permanent harm.
What Is Lewy Body Dementia?
Lewy Body Dementia is an umbrella term that includes two related conditions: Dementia with Lewy bodies (DLB) and Parkinson’s disease dementia (PDD). Both are caused by abnormal deposits of alpha-synuclein protein in brain cells.
The Hallmark Symptoms
- Cognitive Fluctuations: Attention and alertness may vary hour-to-hour (often mistaken for delirium).
- Visual Hallucinations: Well-formed, recurrent visual hallucinations appear early on.
- REM Sleep Behavior Disorder (RBD): Acting out dreams—sometimes years before cognitive decline.
- Parkinsonism: Slowness, rigidity, and gait instability coexisting with cognitive changes.
Why Misdiagnosis is Dangerous
Up to 50% of patients with LBD experience severe reactions to antipsychotic medications, including life-threatening rigidity or neuroleptic malignant syndrome. Many patients are initially misdiagnosed with Alzheimer’s or Parkinson’s, leading to the use of drugs that are unsafe for the LBD brain.
Case Study: A Preventable Crisis A 72-year-old man was treated with a standard antipsychotic for hallucinations before his LBD diagnosis. Within days, he developed profound rigidity and became unable to walk. This highlights why accurate diagnosis must come before heavy medication.
🌳 Interactive Decision Tree: Is This Therapy Right?
Use this logic flow to navigate care decisions with your neurologist:
- Are hallucinations distressing or dangerous?
- No → Use non-drug strategies and environmental changes first.
- Yes → Continue to step 2.
- Has LBD been confirmed or strongly suspected?
- No → Request a full neurologic evaluation before starting any psychiatric drugs.
- Yes → Continue to step 3.
- Is an antipsychotic being considered?
- Yes → Ask your doctor: “Which agents are safest in LBD, and what is the lowest possible dose?”
- No → Explore cholinesterase inhibitors (like Donepezil) first.
🧬 The “Vagus Highway”: How the Gut Influences LBD In 2026, we understand that a “leaky” gut barrier does more than cause digestive upset; it allows pro-inflammatory lipopolysaccharides (LPS) to enter the bloodstream, triggering systemic inflammation that weakens the blood-brain barrier.
Synuclein Seeding: Research shows that chronic gut inflammation can cause alpha-synuclein to misfold in the intestinal lining. These misfolded proteins then use the vagus nerve as a highway to reach the brain’s cognitive centers.
The GLP-1 Connection: Modern therapies like GLP-1 agonists (often used for metabolic health) are being studied for their “neuroprotective” effects, as they help stabilize the gut barrier and reduce the “fire” in both the gut and the brain.
🦠 The Gut-Brain Axis: The “Bottom-Up” Origin of LBD
Recent 2026 studies suggest that LBD may begin in the gut years before the first hallucination or “mini-stroke” symptom appears. This is known as the Enteric Origin Hypothesis.
🧪 2026 Microbiome Targets
To protect the brain, we must first protect the gut lining. Clinical research now focuses on these specific targets:
- Akkermansia Muciniphila: A “keystone” bacteria that strengthens the mucus lining of the gut. Low levels are frequently seen in patients with early-stage LBD and Parkinson’s.
- Short-Chain Fatty Acids (SCFAs): Produced by fermenting fiber, SCFAs like Butyrate act as a direct fuel source for brain-protective cells (microglia).
- The “Leaky Gut” Marker: High levels of Zonulin in the blood can indicate a compromised barrier, signaling a higher risk for neuro-inflammation.
Researcher Tip: Managing the Gut-Brain axis is why target protein intake (1.2–1.5 g/kg) and high-fiber “Prebiotic” foods are non-negotiable for LBD patients in 2026.
###📊 2026 Gut-Brain Nutrition Table#
| Nutrient | Target Purpose in LBD | 2026 Food Source |
| Polyphenols | Reduces oxidative stress in the gut | Blueberries, Green Tea, Extra Virgin Olive Oil |
| Resistant Starch | Boosts Butyrate (SCFA) production | Cooked and cooled potatoes/rice, green bananas |
| Targeted Probiotics | Lowers “systemic fire” (CRP)Fermented foods (Kimchi, Kefir) or specific LBD strains |
Treatment: What Actually Helps
| Symptom Type | Recommended Approach | Risk Note |
|---|---|---|
| Cognitive | Cholinesterase inhibitors (Rivastigmine) | First-line for alertness and hallucinations. |
| Movement | Low-dose Levodopa | Can worsen hallucinations; must be balanced. |
| Sleep | Melatonin & Sleep Safety | Avoid heavy sedatives which increase fall risk. |
Senior Questions & FAQ
Why does LBD fluctuate so much? LBD affects the brain networks controlling attention. This leads to sudden shifts in thinking and awareness throughout the day.
Are hallucinations always psychiatric? No. In LBD, they are neurologic—caused by changes in the visual-processing parts of the brain, not a psychiatric illness.
Is LBD common? Yes. It is the second most common degenerative dementia after Alzheimer’s, despite being underdiagnosed.
March 2026 Clinical Update Current advocacy for liver health emphasizes high-protein intake (1.2-1.5 g/kg) to prevent sarcopenia. Portal hypertension targets for esophageal or gastric varices now align with a systemic blood pressure of <130/80 mmHg.
📘 Related Patient Resources
- The Log: Start tracking “Clarity Scores” with my Daily Glucose & Wellness Tracker.
- The Foundation: New to research? Read the Beginner’s Guide to Metabolism.
- Early Detection: New biomarkers for ALS and FTD.
Clinical References
- Mayo Clinic: Diagnosis and Management of LBD
- PubMed: Fourth Consensus Report on DLB (2025/2026 Update)
- LBDA.org: Comprehensive Treatment Strategies