Heart Health in Later Years: Managing Valve Disease and Biological Aging
Exploring the rise of silent valve disease, the clinical debate over statins in the elderly, and how 2026 research is targeting the mechanisms of biological aging.

Understanding Age-Related Heart Risks
As we age, our bodies undergo inevitable shifts, making heart health a primary focus for older adults. In the United States, heart disease remains the leading cause of death, with seniors particularly vulnerable to its complications.
This research update explores the rise of silent valve disease, the debate surrounding statin use in the elderly, and how emerging therapies are targeting the root causes of biological aging.
Medical Disclaimer: This content is for informational and educational purposes only. It does not replace professional medical advice, diagnosis, or treatment. Always consult a qualified healthcare provider regarding any medical condition.
Figure 1: Cardiovascular resilience in senior years depends on a combination of movement, metabolic stability, and clinical oversight.
The Physiological Shifts of Aging
With age, arterial elasticity naturally reduces and heart muscle walls often thicken. One primary driver is atherosclerosis, where fatty deposits (plaque) accumulate in arterial walls, narrowing blood flow to critical organs and increasing the risk of heart attacks and strokes.
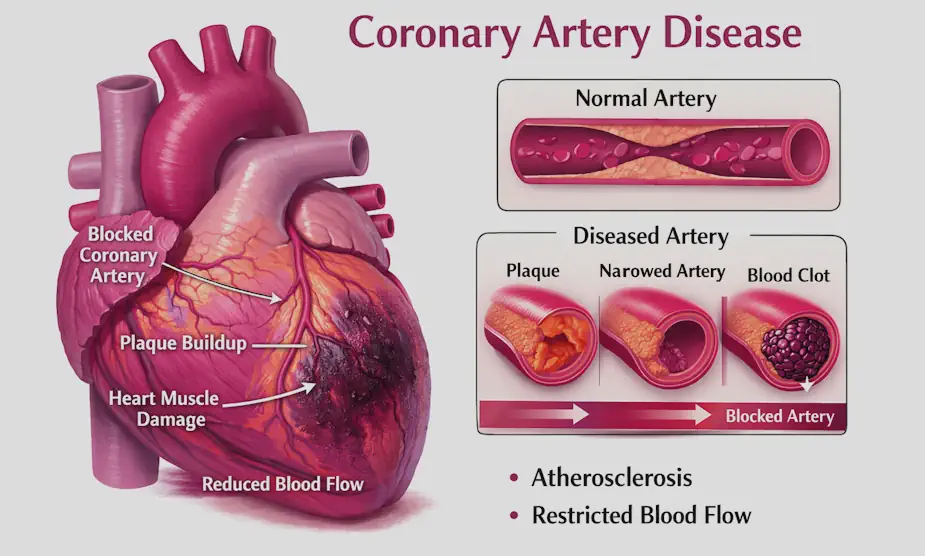
Figure 2: Coronary artery disease occurs when plaque buildup narrows the arteries that supply blood to the heart, reducing oxygen flow.
The Hidden Burden of Valve Disease
Heart valves that control blood flow can become stiff (stenosis) or weak (regurgitation) over time. Recent data indicates that over one in four seniors are affected by asymptomatic valve disease—conditions that show no outward symptoms but pose a significant risk of heart failure.
- The Progression: Prevalence jumps from 21% in those aged 60–64 to over 53% in those 85 and older.
- The Warning Sign: Often, the first sign isn’t pain, but a subtle “fatigue” that seniors often mistake for “just getting older.”
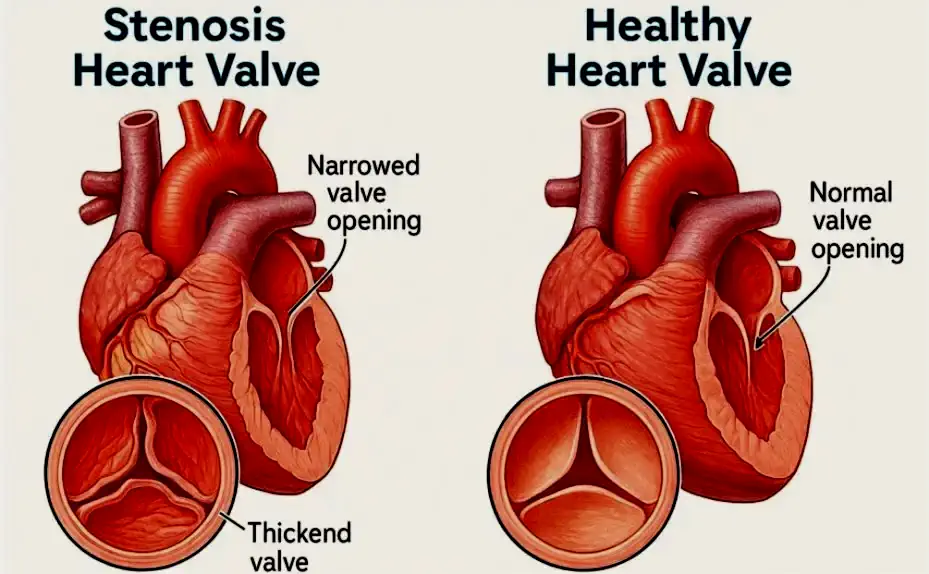
Figure 3: A healthy valve (left) opens fully. A stenotic valve (right) becomes calcified and narrowed, forcing the heart to work harder to maintain systemic circulation.
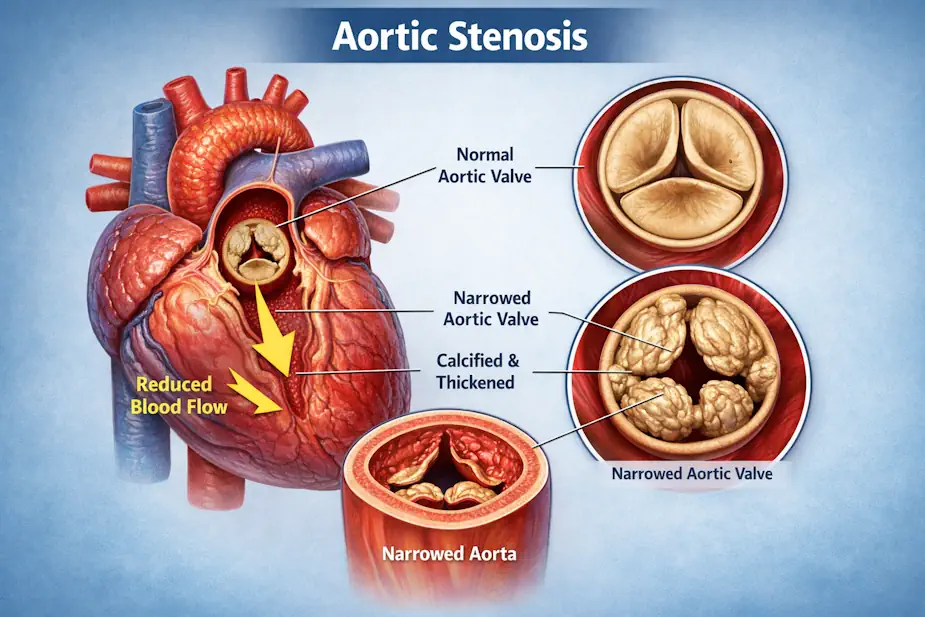
Figure 4: Aortic stenosis occurs when the aortic valve becomes thickened and calcified, narrowing the opening and forcing the heart to pump harder.
Statins for the Elderly: A Clinical Perspective
Statins are the standard for lowering cholesterol and preventing plaque buildup. However, their use in the “very old” remains a point of clinical discussion, particularly regarding quality of life versus longevity.
The Statin “Side-Effect” Reality
While statins are proven to reduce heart attack and stroke risk, they are not universally tolerated.
- Myalgia: Many seniors experience severe leg and muscle cramps (myalgia) that can impact mobility.
- The Balance: Statin therapy should be a tailored conversation. If side effects prevent a senior from exercising (a primary pillar of health), the “net benefit” of the medication may need to be re-evaluated by their care team.
🎯 March 2026 Clinical Update: Resilience Targets
- Blood Pressure: To protect the delicate cerebral and cardiac micro-vasculature, the 2026 target for seniors is now <130/80 mmHg.
- Protein Support: To combat sarcopenia and support the mechanical repair of heart tissue, seniors must target 1.2–1.6 g/kg of high-quality protein (USDA 2026).
- Vascular Integrity: Maintaining these targets is essential for those managing Type 3 Diabetes pathways or Liver Pressure.
🧬 Research Frontier: Targeting Biological Aging
Current treatments effectively manage the symptoms of heart disease, but the frontier of 2026 cardiology is shifting toward addressing the mechanisms of aging itself.
- Cellular Senescence: Researchers are exploring “Senolytics”—drugs that clear out “zombie cells” that cause systemic inflammation.
- Epigenetic Reversal: Healthy behaviors (The Big 6 Pillars) are now clinically proven to “turn back” the biological clock of heart cells.
- Metabolic Repair: Using medications like GLP-1s not just for weight, but for their direct vascular protection properties.
🔬 The Structural vs. Vascular Difference
It is possible to have perfectly “clean” arteries (no plaque) but still suffer from Stenosis or Valve Disease. While statins and diet target the plaque, structural issues often require mechanical monitoring like an Echocardiogram. If you are experiencing unexplained shortness of breath despite stable glucose and blood pressure, ask for a structural heart check.
About the Researcher
Tommy T. Douglas is an independent health researcher and patient advocate. A survivor of a major heart attack (2008) who manages Type 2 Diabetes, he specializes in translating complex cardiovascular data into actionable health literacy for the aging population.
🧩 Clinical Research Glossary
Scientific Sources
- AHA Heart Disease Statistics (2025 Update).
- European Heart Journal (2024): Prevalence of Asymptomatic Valvular Heart Disease in the Elderly.
- Cardiovascular Research (2025): Anti-ageing interventions for Cardiovascular Disease.